Transforming Growth Factor-β Signaling Pathway in Patients With Kawasaki Disease
Chisato Shimizu, MD, at al.
Circulation: Cardiovascular Genetics. 2011; 4: 16-25
Background— Transforming growth factor (TGF)-β is a multifunctional peptide that is important in T-cell activation and cardiovascular remodeling, both of which are important features of Kawasaki disease (KD). We postulated that variation in TGF-β signaling might be important in KD susceptibility and disease outcome.
Methods and Results— We investigated genetic variation in 15 genes belonging to the TGF-β pathway in a total of 771 KD subjects of mainly European descent from the United States, the United Kingdom, Australia, and the Netherlands. We analyzed transcript abundance patterns using microarray and reverse transcriptase–polymerase chain reaction for these same genes, and measured TGF-β2 protein levels in plasma. Genetic variants in TGFB2, TGFBR2, and SMAD3 and their haplotypes were consistently and reproducibly associated with KD susceptibility, coronary artery aneurysm formation, aortic root dilatation, and intravenous immunoglobulin treatment response in different cohorts. A SMAD3 haplotype associated with KD susceptibility replicated in 2 independent cohorts and an intronic single nucleotide polymorphism in a separate haplotype block was also strongly associated (A/G, rs4776338) (P=0.000022; odds ratio, 1.50; 95% confidence interval, 1.25 to 1.81). Pathway analysis using all 15 genes further confirmed the importance of the TGF-β pathway in KD pathogenesis. Whole-blood transcript abundance for these genes and TGF-β2 plasma protein levels changed dynamically over the course of the illness.
Conclusions— These studies suggest that genetic variation in the TGF-β pathway influences KD susceptibility, disease outcome, and response to therapy, and that aortic root and coronary artery Z scores can be used for phenotype/genotype analyses. Analysis of transcript abundance and protein levels further support the importance of this pathway in KD pathogenesis.
Showing posts with label Kawasaki. Show all posts
Showing posts with label Kawasaki. Show all posts
Tuesday, February 15, 2011
Wednesday, January 5, 2011
General Cardiology: Kawasaki - Non-coronary Cardiac Involvement in Acute Kawasaki
| J Am Coll Cardiol, 2011; 57:86-92, © 2011 by the American College of Cardiology Foundation |
Noncoronary Cardiac Abnormalities Are Associated With Coronary Artery Dilation and With Laboratory Inflammatory Markers in Acute Kawasaki Disease
Objectives: We explored the association of noncoronary cardiac abnormalities with coronary artery dilation and with laboratory inflammatory markers early after Kawasaki disease (KD) diagnosis.
Background: Left ventricular (LV) dysfunction, mitral regurgitation (MR), and aortic root dilation occur early after diagnosis; their associations with coronary artery dilation and inflammatory markers have not been well-described.
Methods: Centrally interpreted echocardiograms were obtained at KD diagnosis and 1 and 5 weeks after diagnosis on 198 subjects in the National Institutes of Health-sponsored Pediatric Heart Network KD pulsedsteroid trial. Regression models were constructed to investigate the relationships among early LV dysfunction, MR, and aortic root dilation with coronary artery dilation and laboratory inflammatory markers.
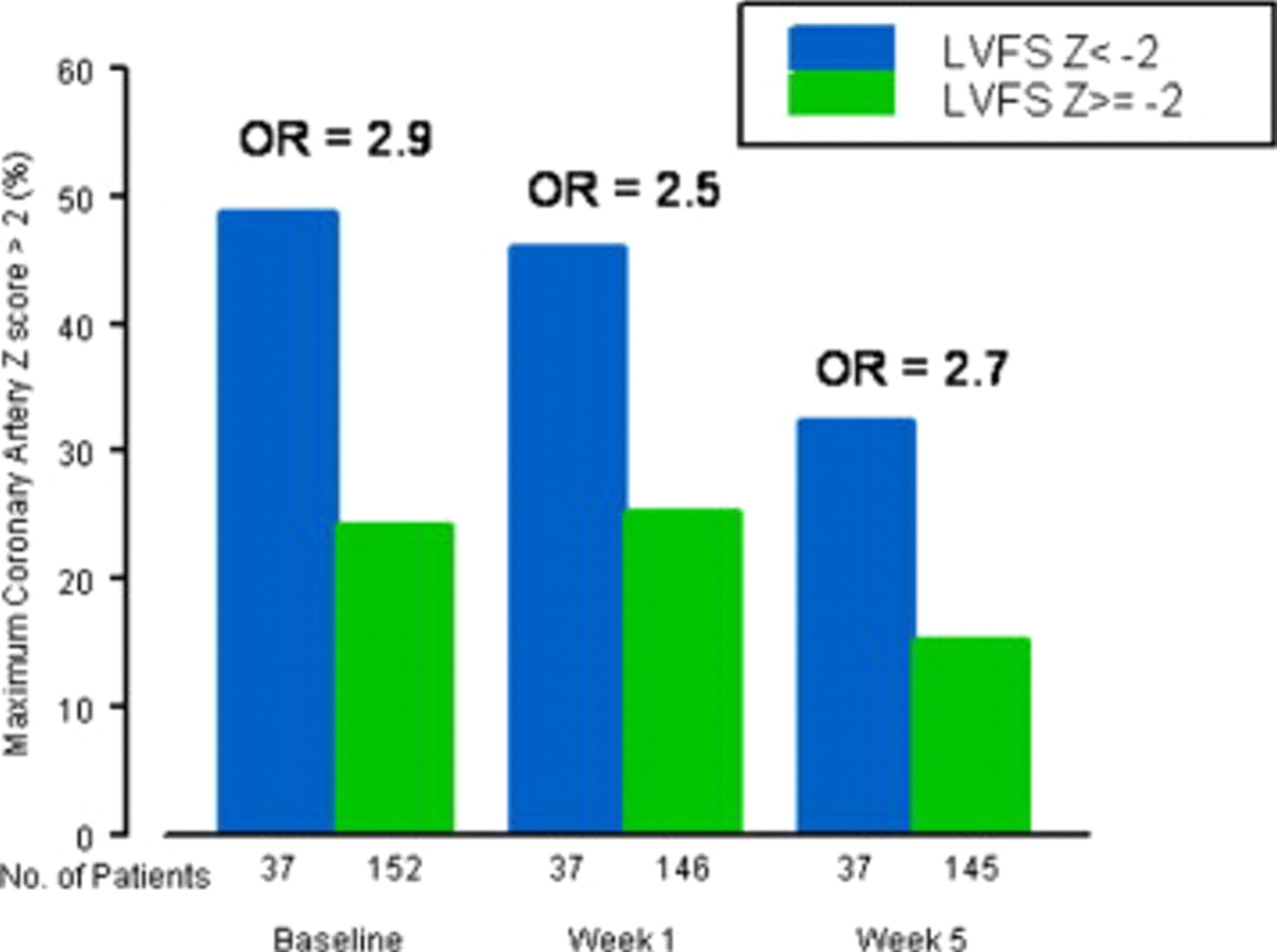
Results: At diagnosis, LV systolic dysfunction was present in 20% of subjects and was associated with coronary artery dilation, seen in 29% (p = 0.004). Although LV dysfunction improved rapidly, LV dysfunction at diagnosis predicted greater odds of coronary artery dilation at 1 and 5 weeks after diagnosis (5-week odds ratio: 2.7, 95% confidence interval: 1.2 to 6.3). At diagnosis, MR was present in 27% of subjects and aortic root dilation was present in 8%; each was associated with larger coronary artery size at diagnosis. Left ventricular dysfunction was associated with higher erythrocyte sedimentation rate and, at diagnosis only, lower serum albumin; MR was associated with higher erythrocyte sedimentation rate and lower albumin at all times. Aortic root size had little association with inflammatory markers.
Conclusions: Noncoronary cardiac abnormalities are associated with coronary artery dilation and laboratory evidence of inflammation in the first 5 weeks after KD, suggesting a shared inflammatory mechanism. (Trial of Pulse Steroid Therapy in Kawasaki Disease [A Trial Conducted by the Pediatric Heart Network]
Subscribe to:
Posts (Atom)